
By Vince Giuliano
Image source The photo shows Nikola Tesla sitting in a building with giant Tesla coils of his own making in 1899, seemingly oblivious of the giant bolts of electricity zapping all around him. This demonstrated the relatively harmless nature of the specific kind of electric current being generated. Later, medical therapy devices were based on the same Tesla technology. See the final photo in this blog entry.
INTRODUCTION
This is a first writeup regarding my recent efforts to seek better understanding the roles of various forms of electromagnetic stimulation on health, longevity and biological processes in general. I focus here centrally on PEMF (Pulsed electromagnetic frequencies) because I have known some things about this technology and its use since the 1970s, and am generally familiar with its purported mechanism of action. I mention my current self-experimentation with PEMF, and have used standard PEMF therapies daily for about a month now. Then, I go on to identify and briefly comment on the alphabet-soup of the other main approaches to electric body simulation. Throughout, I refer to specific systems used. Finally, I relate an anecdote about my first deep involvement with a medical electrical stimulation device.
As context, Steve Buss and I have been concerned with a family of health-inducing and age reversal processes which we have called YOUNGING1.0. We have generated a number if blog entries about this and it has been the subject of our recent webcast on YOUNGING -Triggering Ancient Mechanisms For Rejuvenation
We have hypothysized and are close to establishing that a common mechanism is found in nearly all living organisms that is part of all restorative and regenerative natural body process. That is the demethylation of the double and triple methylated histone H3K27me2-3 by the histone deacetylase JMJD3. Further, we have asserted that this same mechanism also a necessary aspect of all effective measures that are life-extending. That is, any effective intervention that promotes rejuvenation will necessarily include enhanced expression of JDJM3. We have, however, yet to establish that expression of JDJM3 is sufficient to induce aspects of age-reversal or YOUNGING1.0.
A number of techniques are known to promote healthfulness and expected longevity and promote the expression of JDJM3. These include systematic exercise, calorie restriction, certain herbal supplements like curcumin, DHEA, infusions of umbilical cord blood plasma, and a few drugs like metformin and rapamycin. We do not yet know the best way to induce expression of JDJM3 so as to safely trigger expression of JDM3 to induce YOUNGING1.0 as a systematic, long-lasting whole-body process.
We do have some strong clues however, and that is to look at techniques that enhance the functioning of the vagal nervous system. Two families of health-generating approaches that that seem underexplored to us in this regard relate, among other matters, to vagal nerve stimulation: 1. Photobiomodulation – the use of red and near and far infrared light, and 2. electromagnetic body stimulation. The results of a round of research on 1. Is reported in the blog entry PRACTICAL INTERVENTIONS FOR YOUNGING1.0 – Part 1 PHOTOBIOMODULATION. This current blog entry reports on a first round of research on 2, focusing on PEMF.
As a general non-technical intro, see The Best Brain Wave Tech Of 2021, part pf the commercial site of one of the equipment vendors. Also you can see History of the most effective PEMF therapy, a YouTube video
PART 1 – PEMF
PEMF – Pulsed electromagnetic frequencies– unlike other electrical therapies, PEMF does not involve electrical connections or direct electrical current flow from the device into the body. Instead, what is involved is transmission of dynamic magnetic variations into the body from electrical coils which do not require direct skin contact. Wound coils, somewhat similar to those found in traditional loudspeakers, are driven by the PEMF device and emanate electrical pulses with programmed frequencies, pulse shapes, durations and intensities for specific therapeutic purposes. the idea here is that there are a number of particular pulse frequencies and characteristics that represent states of the nervous system, and that such states can to significant extents be induced by external pulse applications at those frequencies. Natural brain and nervous system signals combine with those of the PEMF device so as to become entrained, that is to become synchronized in period and phase so as to reinforce one another.
Particularly there are certain well known brain wave frequencies
| Frequency band | Frequency | Brain states |
| Gamma | 30-100Hz | problem solving, deep thinking, happiness |
| Alpha (α) | 8–12 Hz | Very relaxed, passive attention |
| Theta (θ) | 4–8 Hz | Deeply relaxed, inward focused |
| Delta (δ) | 0.5–4 Hz | Sleep |
In a nutshell, Alpha brainwaves relate to creativity and daydreaming, Beta waves are produced in the middle of deep thinking, Delta/Theta waves can be found during deep sleep, and Gamma waves are associated with problem solving, happiness, and compassion.
Source of following materials on brain waves is NeuroHeath Brainwaves – The Language
“DELTA (0.1 to 3.5 Hz)
The lowest frequencies are delta. These are less than 4 Hz and occur in deep sleep and in some abnormal processes. It is the dominant rhythm in infants up to one year of age and it is present in stages 3 and 4 of sleep. It tends to be the highest in amplitude and the slowest waves. We increase Delta waves in order to decrease our awareness of the physical world. We also access information in our unconscious mind through Delta. Peak performers decrease Delta waves when high focus and peak performance are required. However, most individuals diagnosed with Attention Deficit Disorder, naturally increase rather than decrease Delta activity when trying to focus. The inappropriate Delta response often severely restricts the ability to focus and maintain attention. It is as if the brain is locked into a perpetual drowsy state. Another way to look at Delta is to imagine you are driving in a car and you shift into 1st gear….you’re not going to get anywhere very fast. So Delta would represent 1st gear,
DELTA (0.1-3 Hz): Distribution: generally broad or diffuse; may be bilateral, widespread. Subjective feeling states: deep, dreamless sleep, non-REM sleep, trance, unconscious. Associated tasks & behaviors: lethargic, not moving, not attentive. Physiological correlates: not moving, low-level of arousal. Effects of training: can induce drowsiness, trance, deeply relaxed states
THETA (4-8 Hz) The next brainwave is theta. Theta activity has a frequency of 3.5 to 7.5 Hz and is classed as “slow” activity. It is seen in connection with creativity, intuition, daydreaming, and fantasizing and is a repository for memories, emotions, sensations. Theta waves are strong during internal focus, meditation, prayer, and spiritual awareness. It reflects the state between wakefulness and sleep and relates to the subconscious mind. It is abnormal in awake adults but is perfectly normal in children up to 13 years old. It is also normal during sleep. Theta is believed to reflect activity from the limbic system and hippocampal regions. Theta is observed in anxiety, behavioral activation and behavioral inhibition. When the theta rhythm appears to function normally it mediates and/or promotes adaptive, complex behaviors such as learning and memory. Under unusual emotional circumstances, such as stress or disease states, there may be an imbalance of three major transmitter systems, which results in aberrant behavior. Back to our car example, Theta would be considered 2nd gear. Not as slow as 1st gear (Delta) but still not very fast.
THETA (3.5-7.5 Hz): Distribution: usually regional, may involve many lobes, can be lateralized or diffuse. Subjective feeling states: intuitive, creative, recall, fantasy, imagery, creative, dreamlike, switching thoughts, drowsy; “oneness”, “knowing.” Associated tasks & behaviors: creative, intuitive; but may also be distracted, unfocused. Physiological correlates: healing, integration of mind/body. Effects of Training: if enhanced, can induce drifting, trance-like state. If suppressed, can improve concentration, ability to focus attention
ALPHA (8-12 Hz): Alpha waves are those between 8 and 12(Hz). Alpha waves will peak around 10Hz. Good healthy alpha production promotes mental resourcefulness, aids in the ability to mentally coordinate, enhances overall sense of relaxation and fatigue. I n this state you can move quickly and efficiently to accomplish whatever task is at hand. When Alpha predominates most people feel at ease and calm. Alpha appears to bridge the conscious to the subconscious. It is the major rhythm seen in normal relaxed adults – it is present during most of life especially beyond the thirteenth year when it dominates the resting tracing. Alpha rhythms are reported to be derived from the white matter of the brain. The white matter can be considered the part of the brain that connects all parts with each other. Alpha is a common state for the brain and occurs whenever a person is alert (it is a marker for alertness and sleep), but not actively processing information. They are strongest over the occipital (back of the head) cortex and also over frontal cortex. Alpha has been linked to extroversion (introverts show less), creativity (creative subjects show alpha when listening and coming to a solution for creative problems), and mental work. When your alpha is within normal ranges we tend to also experience good moods, see the world truthfully, and have a sense of calmness. Alpha is one of the brain’s most important frequency to learn and use information taught in the classroom and on the job. You can increase alpha by closing your eyes or deep breathing or decrease alpha by thinking or calculating. Alpha-Theta training can create an increase in sensation, abstract thinking and self-control. In our car scenario, Alpha would represent neutral or idle. Alpha allows us to shift easily from one task to another.
ALPHA (8-12 Hz): Distribution: regional, usually involves entire lobe; strong occipital w/eyes closed. Subjective feeling states: relaxed, not agitated, but not drowsy; tranquil, conscious associated tasks & behaviors: meditation, no action. Physiological correlates: relaxed, healing. Effects of Training: can produce relaxation. Sub band low alpha: 8-10: inner-awareness of self, mind/body integration, balance. Sub band high alpha: 10-12: centering, healing, mind/body connection
BETA (above 12 Hz) Beta activity is ‘fast’ activity. It has a frequency of 14 and greater Hz. It reflects desynchronized active brain tissue. It is usually seen on both sides in symmetrical distribution and is most evident frontally. It may be absent or reduced in areas of cortical damage. It is generally regarded as a normal rhythm and is the dominant rhythm in those who are alert or anxious or who have their eyes open. It is the state that most of brain is in when we have our eyes open and are listening and thinking during analytical problem solving, judgment, decision making, processing information about the world around us. Beta would represent overdrive or hyperdrive in our car scenario. The beta band has a relatively large range, and has been divided into low, midrange and high.
LOW BETA (12-15HZ): Distribution: localized by side and by lobe (frontal, occipital, etc). Subjective feeling states: relaxed yet focused, integrated. Associated tasks & behaviors: low SMR can reflect “ADD”, lack of focused attention. Physiological correlates: is inhibited by motion; restraining body may increase SMR. Effects of Training: increasing SMR can produce relaxed focus, improved attentive abilities,
MID BETA (15-18hz): Distribution: localized, over various areas. May be focused on one electrode. Subjective feeling states: thinking, aware of self & surroundings. Associated tasks & behaviors: mental activity. Physiological correlates: alert, active, but not agitated. Effects of Training: can increase mental ability, focus, alertness
HIGH BETA (above 18hz): Distribution: localized, may be very focused. Subjective feeling states: alertness, agitation. Associated tasks & behaviors: mental activity, e.g. math, planning. Physiological correlates: general activation of mind & body functions. Effects of Training: can induce alertness, but may also produce agitation.
GAMMA (above 30 Hz) Distribution: very localized. Subjective feeling states: thinking; integrated thoughts. Associated tasks & behaviors: high-level information processing, “binding.” Physiological correlates: associated with information-rich task processing. Effects of Training: not known. Gamma is measured between 30 and 44 (Hz) and is the only frequency group found in every part of the brain. When the brain needs to simultaneously process information from different areas, its hypothesized that the 40Hz activity consolidates the required areas for simultaneous processing. A good memory is associated with well-regulated and efficient 40Hz activity, whereas a 40Hz deficiency creates learning disabilities.”
SEE https://omnipemf.com/product/neorhythm/?wcpbc-manual-
 The NeoRhythm PEMF device offers these custom frequencies and predefined programs:
The NeoRhythm PEMF device offers these custom frequencies and predefined programs:
Custom Frequencies (NeoRhythm)
- Delta brainwaves (sleep, meditation)
- Theta brainwaves (meditation, relaxation)
- Alpha brainwaves (relaxation, regeneration)
- Beta brainwaves (focus, general well-being)
- Gamma brainwaves (awarness, memorizing)
Predefined Programs (NeoRhythm)
The Neorhythm device also allows advanced users to create their own custom PEMF program through specifying a dominant frequency and associated magnetic flux density and an accompanying frequency and associated magnetic flux density, For example, these values for four of the default Neorhythm programs are:
PAIN CONTROLDominant frequency: 303 Hz |
ENERGY & VITALITYDominant frequency: 40.5 Hz |
DEEP RELAXATIONDominant frequency: 10 Hz |
LUCID DREAMINGDominant frequency: 40 Hz |
Two small-scale double blind placebo-controlled clinical studies related to the NeoRhythm device are:
- Relaxation study: https://www.researchgate.net/pub…
- Attention study: https://www.researchgate.net/pub…
 The Hapbee PEMF device appears to offer a different kind of flexibility, but at additional cost for a Hapbee membership. Hapbee claims to associate PEMF signal patters with bioactive molecules.
The Hapbee PEMF device appears to offer a different kind of flexibility, but at additional cost for a Hapbee membership. Hapbee claims to associate PEMF signal patters with bioactive molecules.
See https://hapbee.com/pages/blendpedia. “A Hapbee Signal is a recording of a molecule’s unique magnetic frequency (such as caffeine). Just choose the blend you’d like to play, and Hapbee projects a low-energy frequency that’s designed to help influence how you feel. Each Blend is designed to imitate the magnetic effects of molecules that people use every day to enchance their mood, get work done, and relax.”
And there are a lot of blends that can be mixed and matched using Hapbee, such as sleep and rest-inducing blends, an alcohol blend, a CBD blend, a chocolate blend, and a nootropic nicotine blend. The idea is that to get access to the effects of a blend of substances to put you in a certain state, say one of being ready for intensive work concentration. Just dial into the PEMF signal pattern that puts you in that state. To get access to the blends you need a Hapbee membership, $19 a month normally although you initially get a month’s access to all blends and choice of two of them when you buy the device. In this regard going with Hapbee is different than going with other devices since your membership costs go on and on and may soon dwarf your original equipment cost.
The Neorhythm and Hapbee devices seem similar and both are currently discounted deeply to the same $249 price point. However the Neorhthtm device puts out significantly higher magnetic flux density: NeoRhythm uses medium-intensity magnetic fields with a maximum magnetic flux density of 20,000-25,000 milliGauss. Hapbee’s peak signal strength is 40 milliGauss–extremely lower although still possibly effective.
PUBLISHED RESEARCH ON THE THERAPEUTIC EFFICACY OF PEMF
When it comes to biological mechanisms of action of PEMF, electromagnetic biological impacts are so ubiquitous and diverse that it is difficult to decide where to start. It is even more difficult to conclude on which impacts are most fundamental and deserve further intense investigation. It is important to bear in mind that all of chemistry, and by extension all of biochemistry, is about electron shells, electrical binding potentials, and electric fields – and therefore is subject to perturbance or modification by EMF fields. So, on the most basic level the impact of PEMF may be extremely complex. Numerous publications have sought to grapple with the complexity and associated possibilities.
For example, back in 2014 the publication BIOLOGICAL EFFECTS OF PULSATING MAGNETIC FIELDS: ROLE OF SOLITONS reported “In this paper, we analyze biological effects produced by magnetic fields in order to elucidate the physical mechanisms, which can produce them. We show that there is a hierarchy of such mechanisms and that the mutual interplay between them can result in the synergetic outcome. In particular, we analyze the biological effects of magnetic fields on soliton mediated charge transport in the redox processes in living organisms. Such solitons are described by nonlinear systems of equations and represent electrons that are self-trapped in alpha-helical polypeptides due to the moderately strong electron-lattice interaction. They represent a particular type of dissipative=less large polarons in low-dimensional systems. We show that the effective mass of solitons is different from the mass of free electrons, and that there is a resonant effect of the magnetic fields on the dynamics of solitons, and, hence, on charge transport that accompanies photosynthesis and respiration. These effects can result in non-thermal resonant effects of magnetic fields on redox processes in particular, and on the metabolism of the organism in general. This can explain physical mechanisms of therapies based on applying magnetic fields.”
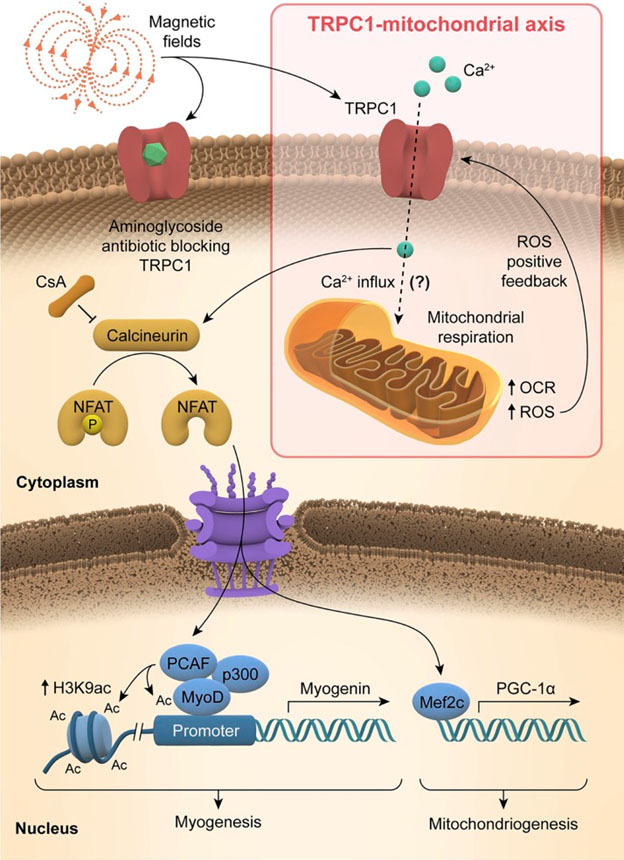
Major impacts of PEMF treatments are thought to be mediated via mitochondria, The 2019 publication Ambient and supplemental magnetic fields promote myogenesis via a TRPC1-mitochondrial axis: evidence of a magnetic mitohormetic mechanism reports: ”We show that both supplemental and ambient magnetic fields modulate myogenesis. A lone 10 min exposure of myoblasts to 1.5 mT amplitude supplemental pulsed magnetic fields (PEMFs) accentuated in vitro myogenesis by stimulating transient receptor potential (TRP)-C1–mediated calcium entry and downstream nuclear factor of activated T cells (NFAT)-transcriptional and P300/CBP-associated factor (PCAF)-epigenetic cascades, whereas depriving myoblasts of ambient magnetic fields slowed myogenesis, reduced TRPC1 expression, and silenced NFAT-transcriptional and PCAF-epigenetic cascades. The expression levels of peroxisome proliferator–activated receptor γ coactivator 1α, the master regulator of mitochondriogenesis, was also enhanced by brief PEMF exposure. Accordingly, mitochondriogenesis and respiratory capacity were both enhanced with PEMF exposure, paralleling TRPC1 expression and pharmacological sensitivity.” This image from that publication illustrates the effect.
Applications of PEMF therapies
The 2016 publication Biological Effects of Pulsed Electromagnetic Field (PEMF) Therapy reports:“Introduction Pulsed electromagnetic field (PEMF) therapy is effective because time-varying or pulsed electromagnetic fields create microcurrents in the body’s tissues. These microcurrents elicit specific biological responses depending on tretment parameters such as amplitude, frequency, and waveform. The body contains multiple electromagnetic fields with each tissue and organ having a unique electromagnetic signature. Computerized Axial Tomography (CAT) scans and Magnetic Resonance Imaging (MRI) scans take advantage of these unique signatures to create a map of the body’s tissues using pulsed electromagnetic fields. While the diagnostic benefits of PEMFs are accepted and widely used, medical practitioners are still realizing the therapeutic benefits of PEMFs. In 1954, Japanese scientists first reported on the piezoelectric properties of bone. This finding led to further research showing that damaged bone responded therapeutically to electric fields and pulsed electromagnetic fields. Then in 1995, scientists at the University of Kentucky found that each type of soft tissue responds favorably to specific electromagnetic frequencies.1 Since then, peer reviewed clinical research documenting the biological and therapeutic effects of PEMFs has increased dramatically. Despite this research contributing to the development of many types of effective PEMF devices, the Food and Drug Administration (FDA) has cleared relatively few of these devices for treating specific conditions. However, as clinical evidence continues to mount, and as patients drive the demand for effective but safer medical therapies, this will likely change. Since the FDA cleared the first therapeutic PEMF device over 30 years ago, there have been no postmarketing safety alerts issued for any of these devices. This reflects the overall safety of short sessions of therapeutic PEMFs. The benefits of PEMF therapy have been documented in multiple peer-reviewed clinical studies for a wide range of medical conditions. Randomized double-blind, placebo controlled clinical trials using PEMF therapy have shown beneficial effects for chronic low back pain, fibromyalgia, cervical osteoarthritis, osteoarthritis of the knee, lateral epicondylitis, recovery from arthroscopic knee surgery, recovery from interbody lumbar fusions, persistent rotator cuff tendinitis, depression, and multiple sclerosis.2,3,4,5,6,7,8,9,10,11 PEMF therapy and current FDA status In 1979, the FDA cleared PEMF therapy in the form of electrical bone growth stimulators for use in treating non-union fractures. Subsequently, the FDA cleared PEMF therapy for failed joint fusion following arthrodesis, failed spinal fusion, and congenital pseudoarthrosis. In 1987, the FDA formally “grandfathered” 510(k) marketing clearance to a high frequency PEMF device for adjunctive therapy in the palliative treatment of postoperative edema and pain in superficial soft tissue. A similar device was given FDA approval in 2008 to deliver what its company calls “targeted microcurrent therapy.” Most recently, in October of 2008, the FDA cleared a PEMF device using repetitive transcranial magnetic stimulation (rTMS) for the treatment of Major Depressive Disorder in adult patients who failed to achieve satisfactory improvement from prior antidepressant medication. In a multicenter clinical trial, approximately half of the patients experienced significant improvement in depression symptoms, and approximately a third of the patients experienced complete symptom relief at the end of six weeks.12 The future of PEMF therapy The future of PEMF therapy is exciting given the findings of early research in a wide variety of health conditions.
For example, preliminary data in clinical studies shows rTMS has promise in treating schizophrenia, post-traumatic stress disorder, obsessive-compulsive disorder, Alzheimer’s disease, and Parkinson’s disease.13,14,15,16,17 In relation to cardiovascular disease, studies show how PEMF therapy may reduce blood glucose levels, blood viscosity, total cholesterol, and triglycerides, while raising high-density lipoprotein (HDL).18,19 These studies will hopefully serve as an impetus for further investigation given that heart disease is the leading cause of death in the United States. Another study shows how PEMF therapy may accelerate the healing of damaged brain tissue following acute stroke. 20 In light of the emergence of drug resistant bacteria, clinical studies show how PEMF therapy could one day become part of the standard of care in inhibiting Staphylococcus aureus infections and augmenting antibiotic therapy.21,22 Complicating the issue of antibiotic resistance are biofilms, dynamic mucous-like cities in which bacteria live and thrive. Biofilms protect bacteria and assist in bacterial cell-to-cell communication and in the exchange of genetic information. The same bacterium living outside a biofilm is less susceptible to antibiotics when living in a biofilm. Studies indicate PEMF therapy may effectively address this dangerous bacterial diversity.23,24
Studies also suggest that PEMF therapy may one day be used to treat cancer. Findings show PEMF therapy induces apoptosis of cancer cells, inhibits the growth of malignant tumors, modulates the immune system via cytokines as an anti-tumor effect, and may act synergistically with chemotherapy and photodynamic therapy to combat tumor growth.25,26,27,28 PEMF therapy and osteoporosis The scientific evidence is accumulating regarding how PEMF therapy may one day gain FDA approval for the prevention and treatment of osteoporosis.29,30 PEMF therapy improves bone mineral density, increase growth of osteoblasts, and positively influence bone remodeling via cytokines, prostaglandins and cell growth factors.31,32,33,34 In the clinical setting, it is important to document objective measures of improvement based on the therapy chosen. Bone density test scores are used to monitor the response to therapy for osteoporosis and osteopenia over the long term. Over the short term, clinicians can use urine deoxypyridinoline (uDPD) levels to monitor response to therapy. Deoxypyridinoline cross links Type 1 collagen found in bone. In conditions where bone turnover is high, deoxypyridinoline spills into the urine in high levels. As bone turnover decreases, uDPD levels drop. In my preliminary analyses, I find that PEMF therapy lowers uDPD in patients with osteoporosis. In one patient, uDPD decreased by 53% in two months with weekly sessions, and the reduction was sustained with once-monthly sessions. If this finding is reproducible in a double-blind, placebocontrolled clinical trial, this would affirm the ability for PEMF therapy to positively impact bone remodeling in osteoporosis.”
The database clinicalrials.gov shows 90 studies for the search term PEMF. Perusing the studies in this list indicates the breadth of conditions that appear to respond to PEMF therapies.
PEMF MECHANISMS OF ACTION
The following diagram from the 2020 publication Promising application of Pulsed Electromagnetic Fields (PEMFs) in musculoskeletal disorders, I think it illustrates some but by far not all of the impacts of PEMF
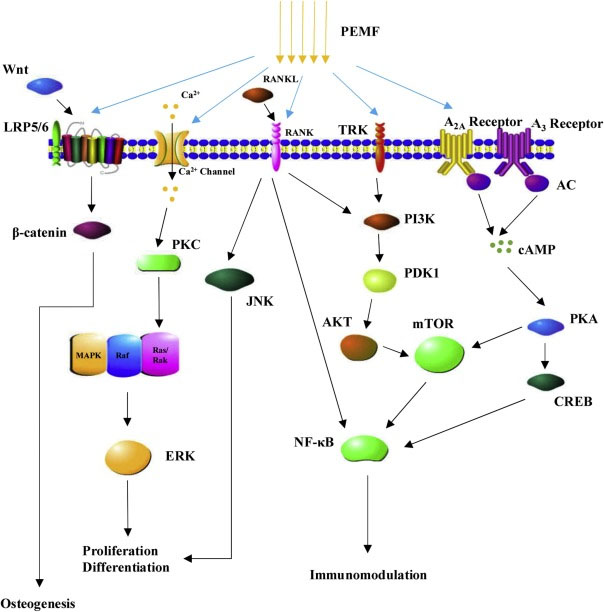
Fig. 1.”The underlying molecular mechanisms of biological effects induced by PEMFs. PEMF stimulation is involved in the regulation of cell proliferation and differentiation as well as immune modulation and inflammation response through a variety of underlying molecular mechanisms.
Abbreviation: PEMFs Pulsed electromagnetic fields; PKC Protein kinase C; MAPK Mitogen-activated protein kinase; ERK Extracellular signal-regulated kinases; RANKL Receptor activator of nuclear factor kappa-B ligand; RANK Receptor activator of nuclear factor kappa-B; JNK c-Jun N-terminal kinase; TRK Tyrosine kinase receptor; PI3K Phosphatidylinositide 3-kinases; PDK1 Phosphoinositide dependent protein kinase-1; AKT Protein kinase “B; mTOR mechanistic target of rapamycin; AC Adenylyl cyclase; cAMP cyclic adenosine monophosphate; PKA Protein kinase A; CREB cAMP response element-binding protein; NF-KB Nuclear factor-kappa B.”
RELATIONSHIP OF PEMF THERAPY TO YOUNGING01
In our writings, Seve Buss and I have characterized YOUNGING01 by a distinctive feature of its mechanism of operation, and that is global histone demethylation of the doubly and triply methylated sites H3K27me3-2 by the specific histone demethylase JDJM3. Large numbers of growth and-development, inflammation-related and other genes related to age-reversal are thus activated. A directly relevant publication is the 2020 Specific low-frequency electromagnetic fields induce expression of active KDM6B associated with functional changes in U937 cells. Recall that KDM6B is a synonym for JDJM3. “In this study, we investigated the effects of specific low-frequency electromagnetic field sequences on U937 cells, an in vitro LFMF model of human monocyte/macrophage differentiation. U937 cells were exposed to electromagnetic stimulation by means of the SynthéXer system using two similar sequences, XR-BC31 and XR-BC31/F. Each sequence was a time series of 29 wave segments, equal to a total duration of 77 min. Here, we report that exposure (4d, once a day) of U937 cells to the XR-BC31 setting, but not to the XR-BC31/F, resulted in increased expression of the histone demethylase KDM6B along with a global reduction in histone H3 lysine 27 tri-methylation (H3K27me3). Furthermore, exposure to the XR-BC31 sequence induced differentiation of U937 cells towards a macrophage-like phenotype displaying a KDM6B dependent increase in expression and secretion of the anti-inflammatory interleukins (ILs), IL-10 and IL-4. Importantly, all the observed changes were highly dependent on the nature of the sequence. Our results open a new way of interpretation for the effects of low-frequency electromagnetic fields observed in vivo. Indeed, it is conceivable that a specific low-frequency electromagnetic fields treatment may cause the reprogramming of H3K27me3 and cell differentiation.”
The U937 call line is a familiar laboratory strain, and the transformation to the m2 anti-inflammatory macrophage phenotype is another aspect of YOUNGING01 we have discussed at length in our blogs. I see two major takeaways from this study: 1. Yes, under certain circumstances PEMF can initiate YOUNGING01 processes, and 2. Careful choice of PEMF parameters such as the difference between XR-BC31 and the XR-BC31/F settings may be required for HOUNGING01 to be activated. We need to understand these a lot better.
Although successful PEMF therapy has been thought to require careful selection of treatment parameters, in most cases how to optimize such parameters to treat a specific disease condition or issue is simply not known. Such parameters include positions of radiating units on the body, pulse waveform (e.g. sinusoidal, sawtooth, triangular, square) pulse frequency and spacing, magnetic field strength, length of treatment sessions, and number of sessions required. As a result, most therapeutic uses of PEMF have been based on heuristic protocols, and we have no idea of how optimal they are.
With respect to PEMF and natural bodily regenerative processes, it appears that there is a fair amount to be said. For example, the 2019 review article The Use of Pulsed Electromagnetic Field to Modulate Inflammation and Improve Tissue Regeneration: A Review reports “Pulsed electromagnetic field (PEMF) is emerging as innovative treatment for regulation of inflammation, which could have significant effects on tissue regeneration. PEMF modulates inflammatory processes through the regulation of pro- and anti-inflammatory cytokine secretion during different stages of inflammatory response. Consistent outcomes in studies involving animal and human tissue have shown promise for the use of PEMF as an alternative or complementary treatment to pharmaceutical therapies. Thus, PEMF treatment could provide a novel nonpharmaceutical means of modulating inflammation in injured tissues resulting in enhanced functional recovery. This review examines the effect of PEMF on immunomodulatory cells (e.g., mesenchymal stem/ stromal cells [MSCs] and macrophages [MΦ]) to better understand the potential for PEMF therapy to modulate inflammatory signaling pathways and improve tissue regeneration. This review cites published data that support the use of PEMF to improve tissue regeneration. Our studies included herein confirm anti-inflammatory effects of PEMF on MSCs and MΦ.”
The publication goes on to cover territory we have covered in other blog entries relating to m1 (pro-inflammatory) and m2 (anti-inflammatory macrophage), pointing out that timely activation of both phenotypes is important for key matters like wound healing and suggesting that PEMF signaling may be key for timely switching of macrophage type expression.
Continuing the selective quote from the document: “The immune system plays an essential role in tissue regeneration following tissue damage as well as during cell signaling homeostasis. The immune response to tissue injury is crucial in determining the efficacy and rate of the healing process, including the extent of scarring and the restoration of organ function.1 To integrate the immune system into regenerative strategies, one of the first challenges is to modulate the precise functions of the different immune components during the tissue healing process. The regulatory interactions of the immune system with tissue regeneration are not unidirectional, and stem cells, as key players in regeneration, can modulate the immune system in several ways to facilitate regeneration.1,2
However, the immune system does not always perform a complementary role in regeneration, and several reports have suggested that increased inflammation can inhibit the regeneration process. An argument can be made that there are immune-mediated mechanisms of regeneration and repair that can be modulated by pulsed electromagnetic field (PEMF) therapy to improve the ability of tissue to regenerate. Until recently, allopathic medicine rejected the possibility that an electromagnetic field (EMF) could affect biochemical mechanisms with weak electrical fields. Biochemistry, however, is based on an understanding of the flow of energy that drives chemical reactions.3
Physical properties of molecules can be combined to express internal energy and thermodynamic potentials, which are necessary for equilibrium and homeostasis in spontaneous processes.4 New models of biophysics emphasize cooperative electrical activity of highly ordered elements at all levels of physiology: cells, tissues, organs, organ systems, as well as the entire human organism. Research has shown that effects caused by low-frequency or weak EMF therapies can induce changes in cell proliferation, alterations in membrane structure and function, changes in nucleic acids, protein phosphorylation and adenosine triphosphate (ATP) synthesis, as well as entrainment of brain rhythms and conditioned brain response in vitro and in vivo.5–7 Parameters of these EMFs include frequency, intensity (field strength), waveform, and time of exposure. Recognition of physiological sensitivities to exogenous EMF came from the observation of endogenous internal electrical processes.4 For example, the piezoelectric properties of bone use electromechanical control to determine either osteoblastic or osteoclastic phenotype of cells.8 However, biophysical properties of cell function have mostly been ignored when choosing treatments for inflammation/immune modulation and regenerative medicine therapies.
Using PEMF to regulate cell signaling mechanisms involved in the inflammatory/immune response pathways of different cell types has become an innovative alternative treatment in the pursuit of regenerative therapies.9,10 Several studies have reported that PEMF can modulate both cell surface receptor expression/activation and downstream signal transduction pathways, thereby restoring homeostatic cell functions such as viability, proliferation, differentiation, communication with neighboring cells, and interaction with components of the extracellular matrix (ECM).11–18 PEMF can activate multiple intracellular pathways, including numerous processes and biochemical mechanisms within both the immune system and tissue regenerative processes, such as the musculoskeletal system7,19,20 and the nervous system.21–23 PEMFs are physical stimuli that affect biological systems through the production of coherent or interfering fields that modify fundamental electromagnetic frequencies generated by living organisms.7,24 These endogenous frequencies are ubiquitous in tissue, for instance, frequencies from 5 to 30 Hz have been found during postural muscle activity (quiet standing) and 10 Hz during walking.25 Successful regeneration requires a balanced immune cell response, with the recruitment of accurately polarized immune cells in an appropriate quantity.2 Here is where PEMF could have an influential role in the inflammatory process and thereby support tissue regeneration.”
PART 2 OTHER ELECTRICAL/ELECTROMAGNETIC STIMULATION APPROACHES
Decoding abbreviations for electrical/electromagnetic stimulation approaches –
E-STIM – E-stim is a general term for the electrical pulses to mimic the action of signals coming from neurons (cells in your nervous system). These mild electrical currents target either muscles or nerves. This is a very generic term. My purpose here is to list the mainline e-stim approaches. I have not studied nor used these approaches so cannot responsiby comment of their efficacy.
Specific types of E-STIM beyond PEMF include:
TENS – transcutaneous electrical nerve stimulation. TENS therapy involves the use of low-voltage electric currents to treat pain. TENS may be used for chronic (long-term) pain as well as for acute (short-term) pain. Electrodes are placed on the skin near the source of the pain. Signals are sen t through nerve fibers to block or at least reduce the pain signals traveling to the brain.
EMS – electrical muscle stimulation. EMS uses a slightly stronger current than TENS to get muscles to contract. The unit’s electrodes (also placed on the skin near the affected muscles) cause rhythmic contractions. This can improve muscle strength if the user attempts to contract the muscle simultaneously. E-stim therapy for muscle recovery sends signals to targeted muscles to make them contract. (Flexing your biceps is a form of muscle contraction.) By causing repeated muscle contractions, blood flow improves, helping repair injured muscles. I own but have not useda VERVE unit that combines TENS and EMF which can be purchased from Amazon.com for $65.
ESTR – Electrical stimulation for tissue repair helps reduce swelling, increase circulation, and speed up wound healing.(ref)
IFC – (Interferential current) stimulates nerves to reduce pain. “Interferential current therapy works by sending small amounts of electrical stimulation to damaged tissues in the body. The therapy is meant to boost the body’s natural process for responding to pain, increase blood flow and the production of hormones that promote healing. — ICT delivers stimulation through two different frequencies, one of about 4000Hz and the other varies up to 400Hz. When the two currents cross, the difference in frequency creates interference, which is where the name for the therapy originates. The exact frequencies, and resulting interferential frequency, can be controlled by the physical therapists during the session. — Interferential current therapy usually requires sessions with a duration of about 9 to 15 minutes. During this time, the physiotherapist will attach four electrode pads to the area which will be treated. Wires connect the pads to the current intensity regulator device which delivers the frequencies required. (ref)
NMES – Neuromuscular electrical stimulation stimulates the nerves in muscles to restore function and strength, prevent muscle atrophy, and reduce muscle spasms. This $65 registered device requires a prescription. Controlled by knobs. From the look of it, suggests a technology of 40 years ago,
FES – Functional electrical stimulation is intended to restore functionality to injured neuromuscular systems, such as due to spinal cord injury. It involves long-term muscle stimulation aimed at restoring function and motor skills. “Functional electrical stimulation (FES) uses small electrical impulses to activate specific muscles and nerves. These impulses trigger the desired function, such as contracting muscles to move a foot or lift an arm. FES is also used to block pain signals and restore or improve bodily functions, such as bowel and bladder control(ref).” FES can involve a number of different hardware approaches, including entire units and/or electrodes implanted in the body. See this document.
SCS – Spinal cord stimulation uses an implantable device to relieve pain.
RSWT radial shockwave therapy See https://www.amazon.com/dp/B082F6HMX1?tag=amz-mkt-chr-us-20&ascsubtag=1ba00-01000-org00-win10-other-smile-us000-pcomp-feature-scomp-feature-scomp&ref=aa_scomp “Radial shockwave therapy (RSWT) is the use of short, intense energy waves travelling faster than the speed of sound. These energy waves stimulate the breakdown of scar tissue and fibroblasts. This process increases blood circulation and initiates metabolic activity, causing an inflammatory response that promotes and stimulates healing. Over the past several years numerous articles and abstracts have been published regarding the effectiveness of RST. Shockwave is clinically proven to have success rates of 91 per cent for calcific tendonitis, 90 percent for plantar fasciitis and 77 percent for tennis elbow.(ref)” My impression is that the shockwaves invove physical molecular movement and not electrical currents, akin to the waves produced by PEMF
ulRFE – ultra low radio frequency “Ultra low frequency (ULF) is the ITU designation for the frequency range of electromagnetic waves between 300 hertz and 3 kilohertz, corresponding to wavelengths between 1000 to 100 km.(ref)” See https://neurohacker.com/the-science-behind-using-ulrfe-technology-to-improve-focused-attention-and-make-you-more-productive.
tDCS – Transcranial Direct Current Stimulation“ Transcranial Direct-Current Stimulation (tDCS) is a portable, wearable brain stimulation technique that delivers a low electric current to the scalp. A fixed current between 1 and 2 mA is typically applied1. tDCS works by applying a positive (anodal) or negative (cathodal) current via electrodes to an area. tDCS is a neuromodulation technique that produces immediate and lasting changes in brain function. The position of the anode and cathode electrodes on the head is used to set how current flows to specific brain regions. The current delivered by tDCS is NOT strong enough to trigger an action potential in a neuron; instead its “sub-threshold” changes the pattern of already activity neurons. Think of the brain as active, trying to do or learn something, and tDCS coming along to boost this ongoing activity. At the cellular level2, tDCS changes neuronal firing and by strengthening synaptic transmission between neurons by augmenting synaptic plasticity3 which is, in turn, the cellular basis of learning. tDCS is often combined with training. Training in itself produces learning (synaptic plasticity), and concurrent tDCS amplifies these effects (enhances synaptic plasticity). Some clinical applications tDCS is currently being explored for are depression, schizophrenia, aphasia, addiction4, epilepsy, chronic pain (migraine, fibromyalgia), attention, and motor rehabilitation. tDCS is also used for non-medical wellness applications, for example accelerated learning5, focus, relaxation, and meditation(ref).6” Also see https://www.google.com/search?q=TDC+devices&oq=TDC+devices&aqs=chrome..69i57.18907j0j15&sourceid=chrome&ie=UTF-8
WB-EMS – whole body electrical myostimulation Suggested for use to halt or reverse sarcopenia, age-related muscle loss. See this page for articles on WB-EMS and devices that induce it. This page points to scientific publications pointing to the benefits and risks of WB-EMS
Clinical multifunctional electrotherapy units – A number of electrical stimulation devices are designed to be used in clinical and professional settings. They maybe used for multiple applications and may cost up to $3,700. For example, this unit offers many electrical as well as sound wave stimulation options
My experience using the Neorhythm PEMF device
About 5 weeks ago when I first started working this blog entry, I surveyed candidate PEMF devices for for my personal use. I was interested in acquiring a practical low-cost device that was known to be efficacious for stimulating the Vagus nerve system and wanted to develop some first-hand experience using PEMF. After looking over the sites for a dozen different brands I ordered a NeoRhythm unit from omnipemf. It was to be used along with my near-infrared and red light belts and Apollo Neuro units. I knew the results I want, which included more concentrated and effective sleep, ability to enhance focus and cognition, and personal energy. I also planned to assess its effectiveness in enhancing HRV and other overnight scores measured by my Oura ring..
The result has been what seems to be very good ability to focus, to be there with family through whatever is going on, and, combined with evening use of my infrared pad, consistently sound sleep. These results appear to be consistent with changes in longstanding patterns observable on my Oura Ring app, namely:
| Monthly overnight average | Nov 2021 | Dec 2021 | Jan 2022 | Feb 1-15 2022 |
| Resting heart rate | 56 | 54 | 55 | 53 |
| Heart Rate Variability | 58 | 72 | 65 | 94 |
| Sleep score | 84 | 87 | 87 | 88 |
| Next-day readiness | 72 | 80 | 81 | 92 |
Higher is better for all scores except resting heart rate where lower is better
Not bad at all,given the results I have been looking for “ which included more concentrated and effective sleep, ability to enhance focus and cognition, and personal energy.” I will see if these results keep continuing with passing time. And I will be looking for additional health benefis of combining therapies with my infrared -red light units, and with my Apollo Neuro unit.
My First Use of a Medical E-Stim Devices
This is a brief historical anecdote about my first personal encounters with a medical e-stim device, 82 years ago when I was ten years old (1940). At the time, a deal friend and family member, had suddenly died, Dr. Joseph DeHoratis, my Godfather. I had occasionally got to rummage unsupervised in the deserted basement in his medical office on Gratiot Ave in Detroit. My grandfather was executor of the Doctor’s estate and I gladly accompanied him when he visited the office to inventory its contents. I headed directly down into the basement, a dark cavernous place full of wonders like a large collection of old medical books with astounding illustrations describing every variety of ailment, immense glass flasks for delivery of IV treatments and who knows what else, and other strange medical contraptions. This time I discovered a mahogany case perhaps weighing 45 pounds which contained an early diathermy machine. Opening the case revealed a marble top, multiple dials and knobs,, and an adjustable spark gap assembly. My grandfather regarded everything in that basement to be junk, and let me take the machine home, where it quickly became part of my developing attic electronics laboratory. The unit generated very high-voltage low-amperage currents in the radiofrequency range. It was based on use of a primitive spark gap and tuning coil apparatus, similar to the first Marconi wireless units used on ocean liners like the Titanic, a version of a Tesla coil. (see initial photo in this blog entry). The high-frequency high-voltage current the unit generated could throw a fat 1.5 inch spark which was harmless to the body because the high-frequency current flowed along the skin. If you held in electrode from the unit in one hand and a fluorescent tube in the other hand, the tube would light up. And anyone touching you would also receive a prickly spark. It was a scary machine worthy of Dr. Frankenstein’s laboratory. The unit I has was a lot like but not quite identical with the one illustrated below here. The knob in the center controlled the adjustable spark gap. One thing the unit could definitely do is destroy all radio reception in the neighborhood. I used the machine often for various “experiments,” and demonstrations to visitors to my laboratory, but never for any actual medical purpose. Later but still when I was a kid, I built more-powerful Tesla machines using both spark-gap and vacuum tube technologies.

