
By James P Watson with editorial assistance from Vince Giuliano
In the style of David Letterman’s “top 10 list” from late night TV, I am listing my own list of the most important things that I personally learned in 2013 about the molecular biology of aging.
Some of the things on this list are not new, but are re-evaluations of “conventional wisdom,” for example anti-aging interventions that were seriously challenged by new objective scientific evidence in 2013. Not every point mentioned in my “top 12 list” were really new for 2013. Rather, they were “new” for me personally, in 2013, as I am learning as much as I can about the molecular biology of aging. Unfortunately, I have had to be willing to accept new evidence that does not always agree with the “conventional wisdom” of yesterday. This always shakes up the establishment and creates lots of angry people who profit from yesterday’s dogma. Fortunately, I am happy to jettison both dogma and dog doo regarding aging. I hope you too will be willing to do so. We must evolve.
1. Reversing Mitochondrial Aging with NAD precursors – The Role of Nuclear NAD deficiency as the Cause of Mitochondrial Dysfunction and Warburg-type Metabolism
In my opinion, this was the “Top Anti-aging Story” of 2013 – The story of how mitochondrial dysfunction is not due to intrinsic mitochondrial degeneration (i.e. the Free Radical Theory of Aging or the Wear and Tear theory) but due to inadequate expression of mitochondrial encoded genes which are controlled by cell nuclear factors. Specifically, when nuclear levels of NAD are low, a sequence of events occurs in the cell nucleus that ultimately results in a lack of adequate expression of mitochondrial DNA genes that are required for Complex I, III, and IV in mitochondrial electron transport. In this scenario, the nuclear-encoded proteins required for mitochondrial electron transport chain are still expressed, but the proteins whose genes are encoded only by mitochondrial DNA are not expressed. Thus, mitochondrial electron transport cannot occur and cells develop a metabolic picture which is typical in cancer, which is called the Warburg effect. With Warburg-type metabolism, cells do not generate ATP from the mitochondria and instead, become dependent on cytoplasmic generation of ATP via aerobic glycolysis.
The primary driver of this “metabolic reprogramming” is the transcription factor, Hypoxia Inducing Factor 1 alpha (HIF-1α), which normally only activates Warburg-type metabolism when oxygen levels are low. Unfortunately, when nuclear NAD+ levels are low, HIF-1α is stabilized and is not degraded by VHL as would normally be the case. As a result, cells are “metabolically reprogrammed” to use aerobic glycolysis in the presence of normal oxygen. HIF-1α inhibits a chain of events that ultimately results in a reduced expression of the mitochondrial transcription factor, TFAM, which normally migrates from the cell nucleus to the mitochondria to stimulate mitochondrial DNA replication. As a result, mitochondrial encoded genes are expressed. When HIF-1α inhibits TFAM, this does not occur. The nuclear encoded mitochondrial proteins are still created via the transcription factor Nrf1, but because TFAM is suppressed by HIF-1α no mitochondrial-encoded protein components of the electron transport chain are expressed. This results in mitochondria that cannot make ATP but still have defective electron transport chains that “run in reverse”. This “reverse electron transport” results in the production of uncontrolled amounts of free radicals from the mitochondria, which then create the “Universal Signature of Aging” which is mitochondrial dysfunction with high free radical production. All of these events can be traced back to inadequate NAD+ in the nucleus. Without adequate NAD+ in the nucleus, SIRT1 cannot function, since NAD+ is a mandatory co-factor for all of the Sirtuins. What David Sinclair and colleagues from both Harvard and Australia showed in a landmark publication late in 2013 was that supplementation with an NAD+ precursor could reverse this mitochondrial dysfunction and “Warburg-like” metabolic state in mice in one week. Sinclair and associates used an NAD+ precursor called NMN, but previous work showed that another NAD+ precursor could also work, Nicotinamide Riboside (NR). NMN is only one step away from NAD+, but is difficult to make and is very expensive. NR is two steps away from NAD+, but is much easier to make, is much less expensive, and is already available for sale under the proprietary name, Niagen. To date, no studies in humans have replicated the findings from Sinclair’s mice studies. Until these are done, we must “hold our breath”. However, in Sinclair’s studies, all of the mitochondrial dysfunction seen in aging mouse skeletal muscle was reversed (with the exception of muscle strength).
In summary, deficiency of NAD+ in the nucleus of muscle cells produces a state of “pseudohypoxia”, where there is adequate oxygen but high levels of HIF-1α. This results in the inhibition of the mitochondrial transcription factor, TFAM, which inhibits the expression of mtDNA. As a result, mitochondria do not produce the proteins encoded in mitochondrial DNA that are required for “forward electron transport” and ATP production. “Reverse electron transport” occurs and high levels of free radicals are produced, giving the exact picture of aging. In this picture cells are dependent on aerobic glycolysis in the cytoplasm and cannot burn fat. They develop the exact metabolic picture of cancer, called the Warburg effect. The mitochondrial dysfunction and this Warburg-type metabolism are fully reversible with the supplementation of NAD+ precursors. This is the #1 story for 2013.

2. Blocking two pathways that drive can produce synergistic effects.
The 2nd most remarkable story in my “Top 10 List” for 2013 was the paper from the Buck Institute that was authored by Di Chen, et al. (Chen, 2013)(ref)(ref) which showed that when both the Insulin/IGF-1 pathway and the mTOR pathway were blocked in nematodes by “genetic knock out,” the nematodes lived 500% longer than normal nematodes. This was a synergistic effect, since genetic knock-out of the Insulin/IGF-1 pathway in nematodes only increased lifespan by 80-100% and genetic knock-out of the mTOR pathway only increased lifespan by 30-40%. However, when both pathways were knocked out, there was a 5-fold increase in lifespan. This dramatic increase was due to cross talk that occurs between the Insulin/IGF-1 pathway and the mTOR pathway via AMPK. AMPK levels dramatically increased in these double knock-out worms and accounted for this synergistic effect. The other component of this synergistic effect was the discovery that the location of this synergistic effect was germline cells, which activated DAF-16 (the nematode homolog of FOXO) in the intestine. Thus, the 5-fold synergistic lifespan extension was attributed not only to AMPK, but also to the fact that DAF-16 regulated fat metabolism in these worms (since intestinal fat is the primary reservoir of fat in nematodes). The diagram below illustrates the lifespan curves of the double-knock out worms, “AMPK crosstalk” between pathways, and the germline-to-intestinal signaling seen in this study:

3. The third story in my “top 10” list is another example of pathway synergy. Combining exercise with Resveratrol supplementation enhances mitochondrial biogenesis more than is explainable due to summing the effects of the individual interventions.
A study Sirtuin 1-mediated effects of exercise and resveratrol on mitochondrial biogenesis published early in the year looked at molecular and biological impacts of combining Resveratrol supplementation with exercise on knockout mice. The findings of the study were:
- Resveratrol (RSV) induces AMPK phosphorylation by 1.7 fold.
- Exercise induces AMPK phosphorylation by 3 fold.
- RSV + Exercise did not have a synergistic effect on AMPK Phosphorylation. The effects of exercise on AMPK were SIRT-independent.
- RSV increased p38 (an MAPK kinase) phosphorylation by 6-fold.
- Exercise increased p38 phosphorylation by 8-fold.
- RSV + Exercise increased p38 phosphorylation by 9.5-fold, which Is not a synergistic effect, The effects of RSV and exercise on p38 were SIRT-independent.
Further:
- Resveratrol (RSV) increased SIRT1 Protein expression by 2-fold,
- Exercise did not increase SIRT1 Protein expression,
- RSV did not increase PGC-1α Protein levels,
- Exercise increased PGC-1α Protein levels by 1.6 fold,
- RSV + Exercise increased both SIRT1 and PGC-1α protein levels, But the increase in PGC-1α was NOT greater than that due to Exercise alone,
- Exercise + RSV synergistically Increased ROS signaling and the Induction of mitochondrial biogenesis That totaled 6.1-fold, whereas with Exercise or RSV alone, the increase was only 3.1 fold or 1.6 fold. This effect was SIRT1 dependent.
Conclusion 1: the effects of Resveratrol and Exercise on AMPK Phosphorylation and p38 MAPK Phosphorylation are SIRT Independent.
Conclusion 2: whereas the AMPK and p38 mediated effects of Exercise and Resveratrol are not dependent on SIRT1, the PGC-1α and ROS-mediated effects of Exercise and RSV are SIRT1 dependent. With Mitochondrial biogenesis, there is a powerful synergistic interaction of Exercise and RSV and this synergistic effect is SIRT1 dependent.
Stories 2 and 3 convey a very powerful message for anti-aging interventions: combining interventions in seemingly independent pathways may produce positive effects that are much greater than additive.
4. We now know what two proteins account for the anti-aging effects of heterochronic parabiosis – GDF-11 (declines with aging) and CCL11 (increases with aging)
My fourth story explains an interesting but unexplainable results previously observed in mouse Heterochronic parabiosis experiments. Heterochronic parabiosis is an old, but novel experimental way of determining if a circulating factor can account for a biological effect by surgically creating a “shared circulation” between two animals. With heterochronic parabiosis (HP), an old animal is surgically connected to a young animal, which allows for a shared circulation to redistribute plasma factors to both animals. Several researchers have used this HP mouse model in the past to study the causes of brain aging, heart aging, and skeletal muscle aging. The diagram below 9;;istrates how HP rejuvenates the older animal. Some rejuvenating factor(s) in the blood of the older animal effectively made the older animal younger in some respects. But that rejuvenating factor(s) was not known. (reference)
I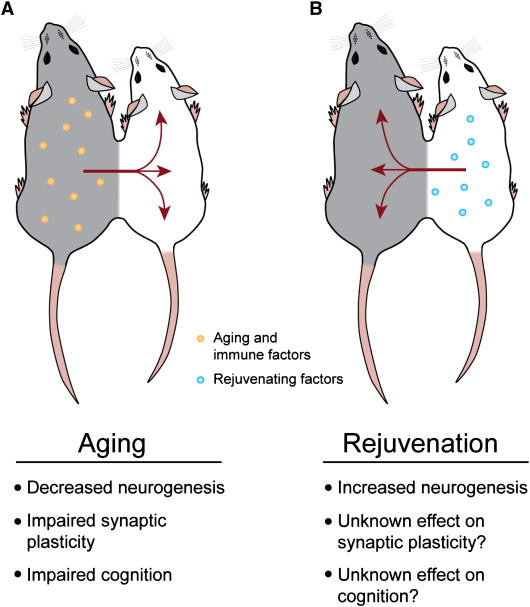
That rejuvenating factor (or at least one of several such factors) was identified in a 2013 publication Growth Differentiation Factor 11 Is a Circulating Factor that Reverses Age-Related Cardiac Hypertrophy by researchers at Harvard Universitiy. They showed that in the heart, the rejuvenation effects of a shared circulation in heterochronic parabiosis could be explained by a circulating protein called Growth and differentiation factor-11. GDF-11 is a member of the TGF-β superfamily of growth factors. It is known that GDF-11 levels decline with aging. (Wagers, 2013). Using a sophisticated experimental technique called “modified aptamer-based proteonomics,” they were able to figure out that this was the protein responsible for reversing the age-related cardiac hypertrophy and diastolic dysfunction seen in the heart with normal aging (often referred to as “normal ejection fraction heart failure). The most convincing evidence was that when this protein was purified and administered to the aging rodents, it recapitulated the effects of parabiosis.

GDF-11 is made by cells found in the spleen. The exact reason why circulating levels of GDF-11 decline with aging has not yet been elucidated, but this is a huge breakthrough.
.Previous studies reported in 2011 used the heterochronic parabiosis model to study brain aging. Using similar techniques, they were able to show that brain aging is due reduce neurogenesis of brain stem cells and that a circulating factor called CCL11/Endotaxin increase with aging. (Villeda, 2011). The data below shows the overlap between the cytokines that are altered with normal aging and the ones that are altered in heterochronic parabiosis experiments(reference):
|
Systemic Chemokine Levels Increase with Aging and Heterochronic Parabiosis and correlate with decreased neurogenesis The Venn diagram that f0llows shows the results of Villeda’s study from 2011. It shows the results of the proteonomic screens where 17 age-related plasma factors correlated strongest with decreased neurogenesis in gray, and 15 age-related plasma factors increased between young isochronic and young heterochronic parabionts in red, and six factors elevated in both screens in the brown are where the circles intersected. This data shows how CCL11 levels increase with age. Thus it appears that CCL11 is a soluble, circulating factor that represses brain neurogenesis. (Villeda, Luo, et al). The aging systemic mileu negatively regulates neurogenesis and cognitive function, Nature, August 31, 477(7362), pp 90-94, 2011
|

Going on to stories about how multivitamin and mineral dietary supplements may be useless
While the four stories above are basically positive, there were a number of negative and partially negative 2013 stories mainly related to antioxidant and vitamin supplementation.
(Vince comment regarding context of these following stories: The research studies behind the stories related below are basically concerned with longitudinal and large-population impacts of vitamin, multi-vitamin and essential mineral supplementation. In interpreting these studies, it is important to keep certain distinctions in mind: 1. While vitamins can be packaged in dietary supplements, many very important dietary supplements are not vitamins, e.g. curcumin, green tea extract, resveratrol, fish oil). It is fallacious to damn vitamin and mineral supplements for not making a difference and then go on to say that all dietary supplements are useless, as is common in the general press. 2. Some vitamins like Vitamin D clearly do make a difference for health as documented by ample other research (actually vitamin D might better be classified as a hormone). 3. Many phyto-substance dietary supplements like curcumin and resveratrol have been broadly and falsely marketed as “antioxidants,” but they in fact primarily operate via epigenetic mechanisms. And many “antioxidant” supplements like alpha-lipoic acid and melatonin were not included in these reported studies; further. they exercise their main benefits via other pathways than direct suppression of ROS. 4. Comparing taking vitamins against eating fresh fruits and vegetables is significant in only one respect. You can’t get the benefits of eating fruits and vegetables from consuming vitamins and minerals because these last substances don’t contain plant-based polyphenols! But you may be able to get some and even more of the benefits of eating fresh fruits and vegetables by consuming other supplements such as green tea extract, resveratrol and curcumin. Back to Jim;s points: I do agree with the general observation that multivitamin and mineral supplementation does not make sense for healthy people who consume well-balanced diets. The message about the general uselessness of multivitamin/mineral supplements is a very important one.)
5. Taking multivitamins or antioxidant supplements does not prevent heart disease
2013 ended with the publication of several studies analyzing the health benefits of multivitamin supplements in large populations over long time periods or in carefully controlled clinical trials. (Fortman, 2013),(Myung, 2013),(Wang, 2013),(Grodstein, 2013), (Vollset, 2013), (Christen, 2013). Since multivatimin and mineral supplements have been the de facto cornerstone of conventional “anti-aging medicine”, it is highly relevant to ANTI-AGING FIREWALLS – THE SCIENCE AND TECHNOLOGY OF LONGEVITY. None of studies mentioned here were funded by Big Pharma, by the FDA, or by the American Medical Association. Instead they were either funded by academia or by peer-reviewed grants from several government agencies in the US, Europe, and Asian countries. (Please, conspiracy theorists, get rid of your paranoia!). Specifically, several were funded by the US Government’s Preventative Services Task Force to obtain objective, unbiased data on the efficacy of multivitamin supplementation for normal, healthy Americans. Specifically, funding was allocated to evaluation supplements for four specific indications: 1) heart disease prevention, 2) cancer prevention – Number 8 in my “top 11” list, 3) prevention of cognitive decline, 4) and for the prevention of a 2nd heart attack. This section covers heart disease. Number 8 in my “top twelve list” will cover cancer prevention. Number 7 will cover cognitive decline, and number 6 will cover the prevention of a 2nd heart attack.
The new meta-analysis data on heart disease prevention
The first new report in 2013 was released online in the November 12 issue of Annals of Internal Medicine (Fortman, 2013). This was a meta-analysis of 26 major multivitamin studies that specifically were designed for preventing chronic disease. The results showed no benefit to taking vitamins and mineral supplements to reduce the risk of heart disease. The 2nd new report in 2013 was from Korea and had no funding from any government agency, trade group, Big Pharma, or FDA (Myung, 2013). This was a meta-analysis of 50 randomized controlled studies involving almost 300,000 research participants who were randomized to receiving multivitamins vs placebo or antioxidant supplements vs placebos. Of all of the outcome measures studied, vitamin and antioxidant supplementation was associated with a marginally increased risk of angina pectoris, whereas low dose vitamin B6 supplementation was associated with a slightly decreased risk of major cardiovascular events. The benefits disappeared in subgroup meta-analysis of high-quality randomized controlled trials within each category, however.
The prospective, randomized, placebo controlled trial for heart disease prevention
A third major study in 2013 looked at the benefits of a multivitamin supplement for preventing heart disease and cancer in male physicians (Gaziano, 2013)(Sesso, 2012). This study was carried out at by the Division of Preventative Medicine at Harvard Medical School and was called the Physicians’ Health Study II (PHSII). The study was a prospective, randomized, double blind, placebo-controlled study in 14,641 male physicians aged 50 or older. They were randomized to a Centrum Silver multivitamin or a placebo. (Centrum Silver is made by Pfizer, a Big Pharma company, and is one of the most popular multivitamin supplements sold). Pfizer did not fund this study and were not involved with the design, execution, or analysis of the data. The follow-up period was 11 years in this study. (The cancer data from this study are reported below under #8). The PHSII showed no cardiovascular risk reduction compared to the placebo. In conclusion, multivitamin supplements for cardiovascular risk reduction “struck out three times” in 2013. Is this consistent with earlier studies published prior to 2013? Read on.
Major studies prior to 2013 that looked at cardiovascular risk and multivitamin supplementation
One must question if the three new 2013 studies were consistent with previous studies that evaluated multivitamin supplements for cardiovascular risk reduction. Two of the largest previous studies reported prior to 2013 were the Women’s Health Initiative (WHI), which was a large cohort study of 161,000 women who were followed for 8 years. The WHI did not show any reduction in cardiovascular risk with multivitamin supplementation (Neuhouser, 2009).
Another large, prospective, randomized clinical trial of Vitamin E supplementation was reported in 2000, called the Heart Outcomes Prevention Evaluation Study (HOPE). This Canadian trial enrolled 2,545 women and 6,995 men aged 55 or older and randomized them to receive 400 IU of Vitamin E vs a placebo for a mean follow-up of 4.5 years (Yusuf, 2000). The results of the HOPE trial showed no statistically significant differences in cardiovascular events or deaths from cardiovascular events in the two arms of the study. The HOPE trial was then extended as the HOPE-TOO trial, which followed 3,994 of the initial patient group who agreed to extend their participation for a mean follow-up of 7 years (Bosch, 2005). The results of the HOPE-TOO trial showed difference in cardiovascular events between Vitamin E and the placebo, but in the Vitamin E group, there was a statistically increased risk of heart failure (RR = 1.13) and hospitalization for heart failure (RR = 1.21).
Conclusion: Old and new studies (2013) consistently show no cardiovascular disease benefit
In conclusion, the WHI study, the HOPE trial, the HOPE-TOO trial, the two meta-analsyis studies from 2013, as well as the Physicians Health Study II all showed the same results. The use of a multivitamin supplement does not reduce your risk of heart disease. On the contrary, all of the researchers involved in these studies emphasize that there is clear, convincing evidence that fruits and vegetables do reduce your risk of cardiovascular disease (Hung, 2004). As Lock said so clearly a few years ago, “if an individual increases fruit and vegetable intake up to 600 gms daily, the worldwide burden of cardiovascular disease could be reduced by 31% for ischemic heart disease and 19% for ischemic stroke”(Lock, 2005). In summary, of all of these researchers agree that you should buy lots of fruits and vegetables for your heart, not supplements for your heart. The only people who strongly disagree with this conclusion are the multivitamin supplement manufacturers, supplement trade groups, and Big Pharma companies that sell multivitamins (Pfizer, Bayer, Novartis, GlaxoSmithKline, Unilever. (Associated Press, 2009). When it comes to taking sides with the supplement/Big Pharma vs the researchers, I could not agree more with the researchers on their conclusions in the above studies.
6. Vitamins and minerals do not prevent a 2nd heart attack
Another major study on multivitamins was released in 2013 that evaluated the benefits of multivitamins and minerals in preventing a 2nd heart attack. (Lamas, 2013). This study was based on data that was extracted from the TACT trial (Trial to Assess Chelation Therapy), which looked at the therapeutic benefit of EDTA chelation therapy (TACT investigators, 2013). This study is very significant in that it was a prospective, double blinded, randomized study comparing a high dose multivitamin and mineral supplement to a placebo. The study was a five-year study involving 1,708 people who had recently had a myocardial infarction within 6 weeks of the time of enrollment. Unfortunately, the researchers found no different in rates of another heart attack, rates of chest pain, hospitalization rates, cardiac catheterization rates, rates of stroke, or early death in placebo vs multivitamin takers. The researchers stated that the interpretation of these results should be taken with caution, since some of the volunteers stopped taking their pills. (This occurs with both the placebo takers and with multivitamin takers).
7. Taking a multivitamin supplement does not help prevent cognitive decline in normal healthy adults, but may prevent cognitive decline in the elderly who have depression
Two major publication evaluating the benefits of a multivitamin supplement on cognitive health have been published in the past two years (one was actually before 2013, but I will include it here). The first study looked at the use of oral folic acid + Vit B12 supplements for the prevention of cognitive decline in older adults aged 60-74 years who had symptoms of depression (Walker, 2012). The primary purpose of supplementation was to see if the folic acid and Vit B12 could prevent cognitive decline in this “at risk” group. The study was a randomized, prospective, placebo controlled study in 900 elderly patients and for this reason, should be taken seriously. The results showed that folic acid and Vit B12 significantly reduced cognitive decline over a two-year follow-up period by 17-18% (p = 0.04 and p = 0.01). This data is consistent with previous reports of folic acid and Vit B12 for these patients.
The 2nd major study evaluated the benefits of a multivitamin on the prevention of cognitive decline in normal, healthy male physicians. It was published online in the December 16 issue of the Annals of Internal Medicine. (Grodstein, 2013). This study was very significant since it was a prospective, placebo-controlled randomized study and was conducted for 12 years in a group of almost 6,000 doctors aged 65 and older. The study randomized the volunteers into a placebo vitamin supplement vs a real multivitamin. All volunteers underwent validated memory testing. At the end of 12 years, there was no effect of the multivitamin in preventing cognitive decline. As a result, the authors, led by Dr. Francine Grodstein of Harvard’s School of Public Health, stated that “this data does not support the use of multivitamin supplements in the prevention of cognitive decline”. It should be noted that this study only looked at cognitive memory testing and not actually the development of dementia. This was very disappointing results, but the study had very few flaws that could be used to discredit it. As predicted, the supplement manufacturers and the Big Pharma both slammed this study as well, since it reduced the sales of supplements by both industries. (Big Pharma actually manufactures as many supplements as the “supplement industry”, even though the “supplement industry” likes to rail against the Big Pharma drug manufacturers). Keep in mind, however, that neither the supplement industry or Big Pharma have been willing to fund studies to counter the scientific conclusions of these papers.
8. Multivitamins reduce cancer risk in males but do not reduce cancer mortality. — Multivitamins may or may not reduce breast cancer risk in females, but eating fruits and vegetables dramatically reduces your risk of cancer in males and females
Prior studies of multivitamins and cancer risk
Prior to 2013, no large-scale, prospective, randomized placebo controlled study of multivitamins for cancer risk reduction had been conducted in the United States. Previous studies were small studies, studies done in other countries, or epidemiologic studies (which are not randomized, blinded, or placebo controlled). The largest US epidemiologic study on multivitamins and cancer risk was the Multiethnic Cohort Study (MEC Study) in the US that involved 215,000 people. The MEC looked at the benefit of multivitamin supplements for cancer risk reduction and showed no benefit. (Park, 2011). The largest randomized study previously reported was an old study conducted in Linxian, China in 1993. Linxian has the world’s highest rates of esophageal/gastric cardia cancer. As a result, death rates from this type of cancer are higher than any other cause of death in Linxian (32% of all deaths are due to esophageal/gastric junction cancer. 2nd highest cause of death is cerebrovascular disease at 25%). In the Linxian study, the researchers were able to show that a mixture of β-carotene, Vitamin E, and selenium reduced cancer rates by 13% and cancer mortality by 9%. In the Linxian study, no reduction in cancer risk was shown with retinol, zinc, riboflavin, niacin, Vitamin C, or molybdenum supplementation (Blot, 1993). The US population in no way resembles the Linxian population, however, since the rates of esophageal/gastric junction cancer are very low in the US.
Multivitamins for cancer risk reduction in males: new data from 2013
With this in mind, the first major report in 2013 regarding cancer prevention with multivitamins was published in May of 2013. (Gaziano, 2013). This was a report summarizing the Physicians Health Study II (PHSII). PHSII was an 11-year, randomized controlled study comparing a multivitamin (Centrum Silver, Pfizer) to a placebo in 14,641 male physicians. The cardiovascular risk outcome was previously reported and described above (Sesso, 2012). The PHS II study was very well designed, with a 12 week placebo run-in period that eliminated non-compliant volunteers. It also stratified participants in the Centrum Silver group and the placebo group to make sure there was a balance in equal age, prior cancer, cardiovascular disease, etc. The study was not sponsored by Pfizer and Pfizer had no say-so in the design or administration of the clinical trial. The primary endpoints were total cancer incidence and major cardiovascular events. All cancer diagnoses were confirmed by pathology report. The median follow-up time was 11.2 years, with 99% follow-up for cancer mortality. The results of the study showed a statistically significant reduction in total cancer incidence (Hazard ratio = 0.92) and total epithelial cell cancer incidence (HR = 0.92). However, the Centrum Silver multivitamins did not reduce cancer mortality or reduce cardiovascular mortality over the 11 year clinical trial period.
In summary, this is the only large prospective study that shows much benefit for the use of multivitamins. Even here, the benefit is very small and only a fraction of the benefit that could be obtained from eating lots of fruits and vegetables (multivitamin = 8% risk reduction in cancer incidence; high fruit & vegetable intake = 20-30% risk reduction in cancer incidence).
Folate, B-vitamins, and Methionine for breast cancer risk reduction in females: new data in 2013
Two small epidemiologic studies were reported in 2013 that looked at folic acid, B vitamins, and methionine and the risk of cancer. The first report in 2013 was a study in 2,325 Hispanic females, where they looked at their dietary intake of folic acid, B Vitamins (B2, B6, B12), and methionine. Although there was no overall association with breast cancer, those that took the most folic acid, B vitamins, and methionine had a lower risk of breast cancer (Yang, 2013).
The 2nd report in 2013 was done by a different group of researchers and looked at the risk of breast cancer in African American females and females of European descent (Gong, 2013).
For African American females, there was a significant correlation between dietary folic acid intake and a risk reduction in premenopausal breast cancer as well as in post menopausal ER+ breast cancer. For American females of European descent, there was no correlation between breast cancer and dietary folate. (Instead, there was a very small increased risk of breast cancer in those that took synthetic folate supplements).
Old data on dietary folate consumption vs folate supplements and breast cancer risk
Previous studies (before 2013) have shown inconsistent results. Some thought that dietary folate consumption reduces breast cancer risk (Shrubsole, 2001)(Maruti, 2009). Other studies have shown no reduction in breast cancer risk with dietary folate consumption (Rohan, 2000). One of the largest studies looking at this association was the Prostate, Lung, Colorectal, and Ovarian cancer screening trial, which looked at 25,400 women and their folate consumption over 10 years. This study showed an 19% increased risk of breast cancer with folic acid supplements but no increased risk with dietary folic acid intake (Stolzenberg-Solomon, 2006). In summary, the data keeps saying the same thing – dietary folic acid is good for you, but taking folic acid supplements may not have any benefit or may even be dangerous.
Older studies (prior to 2013) of multivitamin supplements and breast cancer risk
There have been several older studies published prior to 2013 that looked at multivitamin supplementation and cancer risk. Some show an increased risk of breast cancer with multivitamin supplement use by as much as 19-33% (Ewertz 1990), (Stolzenberg-Solomon, 2006). Other studies have shown no increase in breast cancer risk or a decrease in breast cancer risk (Nagel, 2010)(Kushi, 1996). However, it should be pointed out that the risk factors of obesity, high fat diet, lack of exercise, high alcohol intake, smoking, and the practice of of estrogen and progesterone hormone replacement therapy in post menopausal breast cancer are so much larger risk factors for breast cancer that at this point, multivitamins are minor issues compared to the “big six” preventable risk factors for breast cancer, which would lower breast cancer risk by 13-23% (Wienecke, 2013)(Friedenreich, 2010).
9. “Enough is Enough” – The case is closed on Multivitamin supplements
The three major papers mentioned above led to an Editorial that was published in the Annals of Internal Medicine on December 16, 2013 (Guallar, 2013). Dr. Edgar Miller, co-author of the editorial and professor of medicine and epidemiology at Johns Hopkins School of Medicine stated that “We believe the case is closed – supplementing the diet of well-nurished adults with (most) mineral or vitamin supplements has no clear benefit and might even be harmful”. He went on to say that “vitamins should not be used for chronic disease prevention. Enough is enough”. They went on to urge consumers to “stop wasting your money on multivitamins”. Instead, they recommended was that consumers spend their money on fruits, vegetables, nuts, beans, low fat dairy, and exercise; which have all been shown over and over and over again in scientific studies to be beneficial in preventing heart disease, cognitive decline, cancer, and recurrent heart attacks. (Unfortunately, this is not what the American public want to hear). As expected, this editorial was visciously attacked by the supplement industry. Steve Mister, president and CEO of the supplement industry lobbying group called the Council for Responsible Nutrition said “It’s a shame for consumers that the authors refuse to recognized the real-life need for vitamin and mineral supplementation, living in a fairy-tale world that makes the inaccurate assumption that we’re all eating healthy diets and getting everything we need from food alone”. Obviously Steve Mister did not read the recommendations of Dr. Edgar Miller – you CAN get all that you need from food….you just have to start eating fruits, vegetables, nuts, and beans instead of pizza, French fries, and burgers! In other words, what I am saying is that no vitamin or mineral will counter-act an unhealthy diet and no exercise. In my opinion, the authors of these studies are right and Mr. Steve Mister is merely trying to defend his industry’s profits.
10. James D Watson weighs in again with insights about cancer
The year 2013 opened with a controversial publication, written by a “Hall of Famer “ in science, James D. Watson (who has also been controversial before). Watson, Crick, and Wilkins won the Nobel Prize in 1962 for deciphering the molecular structure of DNA. For the past 50 years, Watson has been studying the genetics of cancer and is unquestionably a leading expert in this field. In January, he published a paper entitled “Oxidants, antioxidants, and the current incurability of metastatic cancers”. Among the many important messages is that Exogenous antioxidants may help cancer survive just as much as they may help you.
In this article, he discussed why science has not won the “War on Cancer”, which was officially started by President Nixon in December, 1971. Step-by-step, he explains the molecular reasons for this failure, and then outlines a plan of how we could “win the war”. In the article, he describes how only several hundred genes out of the 21,000 human genes account for cancer development by “driving” cell growth and division via growth-factor-induced signal transduction pathway up-regulation. This is accompanied by the evasion of programmed cell death (apoptosis resistance), which is the primary reason for why cancer cells are initially resistant to chemotherapy and radiation therapy. Cross talk between these growth factor induced signal transduction pathways develop as more and more DNA mutations occur. This cross talk activates new signal transduction pathways when existing pathways are blocked by a single drug. (An example is the resistance that develops with melanoma against the drug Zelboraf, which blocks BRAF, yet cancers become resistant to it). Another reason for drug resistance is due to changes in the epithelial-to-mesenchymal transition (EMT) that occurs with cancer due to the hypoxic surrounding environment, which induces the “VGEF/HIF-1α driver pathway” for EMT activation. It is this EMT activation that “drives” the development of “cancer mesenchymal cells” which have also been referred to as “cancer stem cells”. Activating the EMT allows cells to loose their attachments to surrounding cells and become free floating. As a result, they can invade and metastasize to a new location. Only when they move to these locations does cancer kill people. This is central to the fundamental molecular biology of cancer.
Note that an evil role for hypoxia and HIF-1α comes up both here and in the inhibition of expression of mitochondrial proteins mentioned in the #1 item above in my 2013 list. That is why I no longer believe in inducing hypoxia as a useful health-inducing hormetic intervention. Vince and I are therefore now closing down the Hypoxia Bar described in our blog entry THE HORMESIS BARS. It appears to be a public health menace.
The link between cancer and aging (and why Aspirin and other anti-inflammatories prevent cancer)
Watson then goes on to explain that while cancer biologist have mainly focused on the Wnt signaling pathway as the primary “early driver” of cancer. there is something else going on too.. Wnt drives β-catenin into the nucleus where it activates the transcription factor TCF to “turn on” the EMT. Watson believes an “even more important villain than Wnt signaling has been virtually staring us in the face for two decades”. That “villain” is interleukin 6 (IL-6). IL-6 is the master cytokine mediator of inflammation and immunity. Recently, IL-6 has also been found to be the principle biomarker for cellular senescence. Specifically, senescent cells secrete the senescence associated secretory phenotype (SASP), which is a group of over 70 cytokines secreted by senescent cells. This explains why the two phenomena, aging and cancer, are chronologically linked. IL-6 can generate paracrine and autocrine feedback loops, thereby activating nearby cells to become cancerous and self-activating the production of more IL-6. This in turn induces apoptosis-resistance by blocking genes required for programmed cell death. It is this IL-6 driven autocrine feedback loop that is blocked by anti-inflammatory drugs like aspirin, COX-2 inhibitors, as well as anti-immune drugs like rapamycin. Thus, a simple way to win the war on cancer would be for everyone to block IL-6 driven signal transduction pathways, which occur early in cancer. These drugs block cell proliferation, not cell division (and are therefore not toxic like chemotherapy drugs that block cell division). This strategy is one Dr. Watson wholeheartedly supports. Thus, he points out preventing IL6-driven autocrine feedback loops is a major goal for cancer prevention
Myc: a “non-linear amplifier” that “drives” late stage, incurable cancer – it must be turned off
Watson then goes on to explain that the transcription factor Myc drives almost every late-stage cancer by up-regulating over 1,000 different genes required for progression through the cell cycle. As a result, Myc may be “an essential feature of much of incurable cancer”. No drugs have been found to effectively block Myc pathways to date, but Watson mentions the discovery of a new way to lower Myc levels – blocking the epigenetic reader protein, bromodomain 4. (BRD4). Specifically, JQ1 is a drug that is a BRD4 inhibitor that was developed for a rare cancer called “NUT midline carcinoma” but as the drug was tested, the researchers noted that Myc levels rapidly plunged. Thus, by blocking this epigenetic reader, BRD4, we may be able to “turn off” Myc in many other common cancers. The interesting thing is that JQ1 actually makes the cancer cells differentiate into macrophages and this is how they block cancer. JQ1 does not block normal macrophage development. Therefore, normal stem cell differentiation is not affected. Using BRD4 inhibitors to down regulate Myc is a strategy that Dr. Watson wholeheartedly supports. Since many different signal transduction pathways activate Myc over-expression, other strategies for turning off Myc were suggested by Dr. Watson as well. Two would be Jak-Stat3 pathway inhibition and HER2-Ras-Raf-Erk3 pathway inhibition. Jak-Stat3 inhibitors would also inhibit IL-6, so there would be a benefit for prevention of early stage cancer as well. For this reason, Watson recommends that we develop many strategies to inhibt Myc.
Why Sleeping prevents cancer via downregulating Myc
Dr. Watson then explains a fascinating finding of how circadian rhythms affect Myc levels. Using RNAi screens of cancer, a specific gene called CSNKe was discovered, which led to the discovery that the circadian clock protein PER2 can act as a tumor suppressor. Specifically, when the PER2 protein is phosphorylated by CSNKe, it undergoes proteasomal degradation. By blocking CSNKe, PER2 selectively binds to DNA promoter sites and turns off many genes, including the MYC gene. Cancer biologist are now starting to develop CSNKe inhibitors, which are a new, promising way of turning off Myc. However, you can do this every night with a good nights sleep as well. This is one explanation of why sleep is so important for cancer prevention.
Why metabolic inhibitors can help us prevent or treat cancer
Dr. Watson then goes on to explain that cancer cells are running at high metabolic rates and are mostly dependent on aerobic glycolysis for generating ATP (i.e. the Warburg effect). This two factors make cancer cells more vulnerable to metabolic inhibitors than normal cells. For this reason, he suggest that we simultaneously use hexokinase inhibitors (which block glycolysis) and mitochondrial inhibitors (which block oxidative phosphorylation). Examples of this would be 3-Bromopyruvate, which block both hexokinase and OXPHOS, or combining 2-deoxyglucose (2DG) and Mito-Q. (2DG blocks hexokinase and Mito-Q blocks OXPHOS). Metabolic inhibitors probably then block cancer via AMPK activation and mTOR inhibition. This is one of the ways that metformin and rapamycin can be used for cancer. Dr. Watson wholeheartedly recommends metabolic inhibition as a way of winning the war on cancer.
There appears to be a contradiction between this recommendation and the suggestion in Story 1 above.. On the one hand, Sinclair et al suggests we want to maintain normal mitochondrial-based metabolism – and that evil and cancer occurs when pseudohypoxia results in such metabolism being blocked leading to glycolysis and the Warburg effect taking over. On the other Hand, James D Watson here is suggesting that to treat cancers we block BOTH glycolysis and normal mitochondrial phosphorylation. It appears that Sinclair wants to keep cells alive and Watson wants to suffocate them. One way to reconcile this is to adopt the first strategy for healthy cells free of cancer and the second strategy once a cancer exists and where the Warburg effect is already operating,
How p53 over expression kills cancer cells by generating ROS
Dr. Watson then goes on to explain that most all effective strategies to kill cancer require increasing p53, which results in a ROS-mediated cell death. Almost all genotoxic chemotherapy drugs increase p53 in cancer cells. In cancers with a functional p53 signaling, this increases the expression of genes that control mitochondrial ROS production. As a result, chemotherapy increases ROS in cancer cells via a p53-mediated, mitochondrial mechanism, thereby causing ROS-induced cell death. In cancers with a non-functional p53 pathway (due to p53 epigenetic silencing or mutations of the p53 gene), effective cancer therapies must directly induce ROS independently of p53. This is why Dr. Watson is “bullish” about the “first in class” ROS generating drug, Elesclomol, which induces ROS independently of p53.
Regardless of whether p53 is functional or non-functional in a cancer, the efficacy of chemotherapy and radiation can be abolished with anti-oxidants like N-acetylcysteine. This has lead many scientists, including Dr. Watson, to enquire if resistant cancers produce their own endogenous antioxidants and if the use of exogenous anti-oxidant supplements were counterproductive. Today the evidence is quite strong – cancer cells do up regulate endogenous antioxidants via the Nrf2 pathway, which is the major reason why these anti-oxidant generating cells are resistant to chemotherapy. Even Elesclomol will not work in these cells. Specifically, cancer cells up regulate the Nrf2 pathway when they are exposed to chemotherapy and radiation therapy. Over-expression of both the RAS and MYC oncogenes in cancer results in up-regulation of Nrf2 because most cancer cells have multiple copies of RAS and MYC that are constitutively “turned on”. This explains much of the confusion over the role of antioxidants in cancer prevention and why they don’t work (see “Top stories” item #8 above). This understanding has solved a major mystery in cancer prevention that has not been previously explained well until Dr. Watson’s article.
Taking exogenous anti-oxidants just help cancer cells survive
All of the above molecular biology is NOT controversial and is well established scientific fact. What is controversial and new about this paper is that James Watson then suggests that “free radical destroying anti-oxidative nutritional supplements may have caused more cancers than they prevented.” By making this statement, Dr. James Watson has again directly attacked the multi-billion dollar supplement industry that uses the term “antioxidant” as a marketing strategy to sell thousands of different kinds of supplements. This attack has brought a lot of opposition from both the $30 billion dollar supplement industry and the $1.2 trillion dollar pharmaceutical industry that also sells multivitamins. (In fact, Big Pharma probably produces more multivitamins than the supplement industry. They make all of the Centrum brand multivitamin supplements). In publishing this paper, Dr. Watson has not suggested that we stop eating fruits and vegetables. Instead, he has challenged the old rationale for eating fruits and vegetables – i.e. they are good for you because they are rich in “antioxidants”. Watson’s paper has generated major backlash from even the nutritional sciences establishment. Despite all this vitriol, the “nutrition establishment,” the supplement industry, and Big Pharma has not provided any good evidence to counter Watson’s views. For this reason, I listed this paper as #10 in my “top 10 list” for 2013. This may end up being #1, ten years from now, however.
11. The only scientifically proven way to lengthen your telomeres is free!
As most of you that read Vince Giuliano’s blogs know, there has been a great deal of interest in telomere lengthening as a way of living longer. In 2013, a landmark study was published that unfortunately went largely unnoticed (Ornish, 2013). In a paper published in August, 2013, Dean Ornish and Elizabeth Blackburn showed that you can lengthen telomeres by 10% over 5 years without pills by merely altering your diet, exercising, and managing your stress. (Even the expensive astragalus supplement made by TA Sciences has been unable to lengthen telomeres. It only reduces the rate of telomere shortening). Elizabeth Blackburn won the 2009 Nobel Prize with Carol Greider and Jack Szostack for discovering telomerease in tetrahymena.
(reference). I think she is a much more credible source of information than the astragalus supplement industry. In this small study, Dean Ornish put a group of elderly males with low grade prostate cancer on a diet that was low in fat (10% of calories), was plant-based (vegan), was high in whole grains, fruits, vegetables, legumes, and was low in refined carbohydrates. (They also had to take one serving of tofu per day and a soy protein powder drink, a selenium supplement, Vitamin C, fish oil, and Vitamin E). They also walked for 30 minutes a day, 6 days per week. The stress management, program including 60 minutes of yoga-based stretching, breathing, meditation, imagery, and progressive relaxation 6 days a week. They also participated in a one hour support group once a week. The study was a 5-year prospective clinical trial with a control group who did not do the above. At the end of the clinical trial, telomere lengths were measured in blood leukocytes and noted to be 10% longer than at the beginning of the trial. On the other hand, the control group had telomeres that were 3% shorter than at the beginning of the trial. This is a remarkable study, considering that no prior study and no supplements have been shown to lengthen telomeres (only reduce the rate of shortening). None of the above interventions are expensive and are not supplement based, except for the selenium, Vitamin C, fish oil, and Vitamin E. (Although it has been shown that exercise and fish oil can affect telomere length, the results of this trial cannot be explained by the fish oil supplements or exercise alone). The conclusion of this study is consistent with the scientific data that supports the idea that telomere length is NOT a biological clock that keeps accurate “biological age” but instead, telomere length is another measure of oxidative stress and that oxidative stress can be managed with lifestyle.
12. Consuming vegetables can impact breast cancer risk
This final story reporting new data from 2013 relates to breast cancer risk as associated with consumption of fruits and vegetables. An analysis study called the Pooling Project of Prospective Studies of Diet and Cancer (Pooling Project) pools the data from multiple published prospective cohort studies. This analysis included the data from 20 studies that met all of the following criteria: At least one publication on any diet and cancer associations, a comprehensive assessment of dietary intake, validation of dietary intake, and stratification of the data by estrogen receptor positivity. This Pooling Project study specifically looked at the effects of fruits and vegetable intake and the risk of ER+ and ER- breast cancer in a pooled population of 993,466 females (Jung, 2013). The results showed no overall reduction in risk of breast cancer, but a statistically significant reduction in ER- breast cancer risk in those who ate vegetables, but no reduction in ER+ breast cancer risk and vegetable intake. Fruit intake did not alter breast cancer risk for either ER+ and ER- subtypes. For the highest quartile of vegetable intake, there was an 18% reduction in the risk of ER- breast cancer (OR = 0.82) but not ER+ breast cancer (OR = 1.04). In summary, this new 2013 paper suggests that vegetables reduce your risk of ER- breast cancers, but not ER+ breast cancer. This is the first study that looked a breast cancer risk reduction separately for ER+ vs ER- cancers, which is a good idea, since the overwhelming “driver” of ER+ breast cancer is estrogen. Thus, it would be difficult to show that fruits and vegetables made a huge difference in ER+ breast cancer. More importantly, this new data is consistent with what we know about other types of cancer and the benefits of eating fruits and vegetables. Specifically, eating fruits and vegetables would reduce the risk of stomach cancer by 19%, the risk of esophageal cancer by 20%, the risk of lung cancer by 12%, and the risk of colorectal cancer by 2% (Lock, 2005). It has been estimated that 2,635,000 deaths per year are due to the inadequate consumption of fruits and vegetables (Lock, 2005).

Hi
I have read Sinclair’s paper and your summary is both concise and astute. There was one part of your discussion that I hadn’t seen there or elsewhere. Namely “This results in mitochondria that cannot make ATP but still have defective electron transport chains that “run in reverse”. This “reverse electron transport” results in the production of uncontrolled amounts of free radicals from the mitochondria, which then create the “Universal Signature of Aging” which is mitochondrial dysfunction with high free radical production. ”
Could you give a reference that gives a clear desciption of why the breakdown of the mitochondrial encoded sub-units cause the electron chain to run backwards and additionally why this produces excessive amounts of free radicals? My background is in physics and my biochemistry is weak at best — the idea of a reverse electron flow is new to me.
Thanks, Jim Rose
I am slowly reading the literature about this mitochondrial renaissance involving NR, NMN or just plain nicotinamide. There is another paper by the people around Guarante that is complementary to the work of Sinclair. Sinclair nails the mechanism for how increasing NAD+ improves mitochondrial OXPHOS. Guarante el al show (1) NR or nicotinamide improve mitochondrial respiration, (2) their mechanism is murky but (3) they show that
feeding NR or nicotinamide to C. Elegans increases lifespan by about 20%.
Also, rather interestingly, they show that PARP1 and CD38 consume NAD+ and can thus contribute to the breakdown of OXPHOS. These compounds implicate DNA repair, immunity and cancer — apparently in competition with healthy OXPHOS. The Guarante paper is Mouchiroud et al. Cell 154, 430-441, July 2013.
jrose:
Good points and I agree a hot topic. Did you see ny latest blog entry NAD+ an emerging framework for life extension — Part 1: The NAD World at
http://www.anti-agingfirewalls.com/2014/11/11/nad-an-emerging-framework-for-life-extension-part-1-the-nad-world-2/
I an familiar with and mention the Guarante paper there.
I am cooking up Part 2 now.
Vince
(Can the human version be blocked with the same lifespan percentage increases? Eric
FGT-1 is the major glucose transporter in C. elegans and is central to aging pathways.
Feng Y, Williams BG, Koumanov F, Wolstenholme AJ, Holman GD.
Author information *Department of Biology and Biochemistry, University of Bath, Bath, BA2 7AY, U.K.
Abstract
Caenorhabditis elegans is widely used as a model for investigation of the relationships between aging, nutrient restriction and signalling via the DAF-2 (abnormal dauer formation 2) receptor for insulin-like peptides and AGE-1 [ageing alteration 1; orthologue of PI3K (phosphoinositide 3-kinase)], but the identity of the glucose transporters that may link these processes is unknown. We unexpectedly find that of the eight putative GLUT (glucose transporter)-like genes only the two splice variants of one gene have a glucose transport function in an oocyte expression system. We have named this gene fgt-1 (facilitated glucose transporter, isoform 1). We show that knockdown of fgt-1 RNA leads to loss of glucose transport and reduced glucose metabolism in wild-type worms. The FGT-1 glucose transporters of C. elegans thus play a key role in glucose energy supply to C. elegans. Importantly, knockdown of fgt-1 leads to an extension of lifespan equivalent, but not additive, to that observed in daf-2 and age-1 mutant worms. The results of the present study are consistent with DAF-2 and AGE-1 signalling stimulating glucose transport in C. elegans and this process being associated with the longevity phenotype in daf-2 and age-1 mutant worms. We propose that fgt-1 constitutes a common axis for the lifespan extending effects of nutrient restriction and reduced insulin-like peptide signalling.
Pingback: NAD+ an emerging framework for life extension — Part 1: The NAD World | AGING SCIENCES – Anti-Aging Firewalls
Pingback: The Hormesis Files: Chronic Ketosis and The Case of The Missing Glutathione | Free The Animal
Eric25001
A great question whose answer as far as I know is unknown. The fact that “knockdown of fgt-1 leads to an extension of lifespan equivalent, but not additive, to that observed in daf-2 and age-1 mutant worms” seems to suggest a whole new viewpoint to this classical approach to nenatode life extension, It suggests to me that in humans a possible matter to look at is the impact of sirtuins on glucose transport. Hmnn!
Vince
I was surprised to see the reference to methionine regarding preventing cancer as I understood it was a significant cause of cancer and one of the biggest problems with eating too much meat. Did I misunderstand something?